
I'm on an ENT (ear, nose, and throat) and ophthalmology (eyes) rotation right now, so I've been doing some thinking about the senses we often take for granted when they work well. That is, I was until this week on night float. But we have a slower week so far, so hence the nighttime blog posts. :)
Seeing
One of my favorite things about ophthalmology has been the simple process of seeing people's eyes being illuminated by the light as the ophthalmologist examines them. The lamp and microscope move in front of their eyes and, at an angle as the ophthalmologist looks at the retina (back of the eye), the light reflects off the whole iris (colored part) in the darkened room, giving the patient these beautifully shining lit-up eyes that reminds me every time of the quote about the eyes being the window to the soul. I am struck by the scene's beauty all the more for the fact that the patient can't see it. Here's this beautifully illumined eye in all its unnoticed complexity, and they have no idea.
 http://mychinaconnection.com/wp-content/uploads/2010/12/see-eye-to-eye.jpg
http://mychinaconnection.com/wp-content/uploads/2010/12/see-eye-to-eye.jpg
Hearing
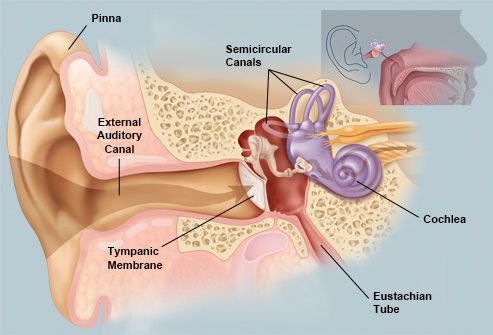
Hearing, too, is affected by things we can't see or access. Even common wax can obstruct one's hearing without the patient knowing what it is that makes them hear less on that side (or both sides). The inner ear itself, where the tiny middle ear bones transmit sound waves made into vibrations that are picked up by microscopic hair cells, is beyond visualization even for the ENT doctor. It can be seen somewhat on a head CT in large scale but the hair cells that may not work as well for hearing as one ages or whose disruption with tiny stones (otoliths) can cause lifestyle-handicapping vertigo (dizziness) are beyond what we can easily access.
 http://www.webmd.com/brain/picture-of-the-ear
http://www.webmd.com/brain/picture-of-the-ear
Hearing and Seeing
In a recent conversation, I was asked which sense I would rather lose - sight or hearing? A difficult question to answer, and one that prompted a quick evaluation of all the taken-for-granted ways these senses affect my life. The crescendo of a piano piece or the steady patter of raindrops. A glorious nearly-neon sunset or the color of sunlight through a leaf. Hearing someone call my name as I walk down the hall. Seeing the identity of the speaker or identifying them by their voice.
Sight and hearing are linked in another way. Both senses require two steps to achieve the appropriate perception of sound/vision. First, the external stimulus must be perceived - cells in the retina send off signals from the eye; those hair cells from the inner ear do the same after the vibrations reach them from the bones of the middle ear. Second, the message received in the brain must be processed appropriately for it to give us the right picture or sound. One needs both steps to actually achieve sight or hearing that is meaningful.
The Bible understands the importance of both of these steps, too. God's judgment on his people when he sends them the prophet Isaiah is: "Be ever hearing, but never understanding; be ever seeing, but never perceiving...Otherwise they might see with their eyes, hear with their ears, understand with their hearts, and turn and be healed" (6:9b-10). This is picked up in the New Testament in Matthew 13 (as well as parallel passages in Mark 4 and Luke 8) when Jesus understands why he speaks in parables, telling stories to communicate truth to those whose ears are open and whose eyes see clearly and concealing it from those who don't.
My experiences on ENT and ophtho make me wonder:
1.) What sort of unseen blockages keep me from hearing God's voice clearly? Pride. Busyness. Independence. For many patients with wax in their ears, simple daily administration of a few drops of oil can help keep the wax soft enough to move out. What similarly mundane practices can help my ears stay open? Daily prayer. Meditation. Time in nature. Time to listen. Cultivating the practice of listening in my relationships. Obedience when I do hear God's direction.
2.) What overlooked glorious beauty and light is shining around me? A simple mirror would enable the patients being examined to see the light illuminating their eyes. How can I be a mirror to others, reflecting the Lord's light to them? How can I be more attentive to God's presence and work in my own life?
 http://stevetallamy.com/wp-content/uploads/2011/04/Seeing-Beauty.jpg
http://stevetallamy.com/wp-content/uploads/2011/04/Seeing-Beauty.jpg
Seeing
One of my favorite things about ophthalmology has been the simple process of seeing people's eyes being illuminated by the light as the ophthalmologist examines them. The lamp and microscope move in front of their eyes and, at an angle as the ophthalmologist looks at the retina (back of the eye), the light reflects off the whole iris (colored part) in the darkened room, giving the patient these beautifully shining lit-up eyes that reminds me every time of the quote about the eyes being the window to the soul. I am struck by the scene's beauty all the more for the fact that the patient can't see it. Here's this beautifully illumined eye in all its unnoticed complexity, and they have no idea.

Hearing
Hearing, too, is affected by things we can't see or access. Even common wax can obstruct one's hearing without the patient knowing what it is that makes them hear less on that side (or both sides). The inner ear itself, where the tiny middle ear bones transmit sound waves made into vibrations that are picked up by microscopic hair cells, is beyond visualization even for the ENT doctor. It can be seen somewhat on a head CT in large scale but the hair cells that may not work as well for hearing as one ages or whose disruption with tiny stones (otoliths) can cause lifestyle-handicapping vertigo (dizziness) are beyond what we can easily access.
Hearing and Seeing
In a recent conversation, I was asked which sense I would rather lose - sight or hearing? A difficult question to answer, and one that prompted a quick evaluation of all the taken-for-granted ways these senses affect my life. The crescendo of a piano piece or the steady patter of raindrops. A glorious nearly-neon sunset or the color of sunlight through a leaf. Hearing someone call my name as I walk down the hall. Seeing the identity of the speaker or identifying them by their voice.
Sight and hearing are linked in another way. Both senses require two steps to achieve the appropriate perception of sound/vision. First, the external stimulus must be perceived - cells in the retina send off signals from the eye; those hair cells from the inner ear do the same after the vibrations reach them from the bones of the middle ear. Second, the message received in the brain must be processed appropriately for it to give us the right picture or sound. One needs both steps to actually achieve sight or hearing that is meaningful.
The Bible understands the importance of both of these steps, too. God's judgment on his people when he sends them the prophet Isaiah is: "Be ever hearing, but never understanding; be ever seeing, but never perceiving...Otherwise they might see with their eyes, hear with their ears, understand with their hearts, and turn and be healed" (6:9b-10). This is picked up in the New Testament in Matthew 13 (as well as parallel passages in Mark 4 and Luke 8) when Jesus understands why he speaks in parables, telling stories to communicate truth to those whose ears are open and whose eyes see clearly and concealing it from those who don't.
My experiences on ENT and ophtho make me wonder:
1.) What sort of unseen blockages keep me from hearing God's voice clearly? Pride. Busyness. Independence. For many patients with wax in their ears, simple daily administration of a few drops of oil can help keep the wax soft enough to move out. What similarly mundane practices can help my ears stay open? Daily prayer. Meditation. Time in nature. Time to listen. Cultivating the practice of listening in my relationships. Obedience when I do hear God's direction.
2.) What overlooked glorious beauty and light is shining around me? A simple mirror would enable the patients being examined to see the light illuminating their eyes. How can I be a mirror to others, reflecting the Lord's light to them? How can I be more attentive to God's presence and work in my own life?



{kind=link}